Ask the internet what dose of progesterone you should take and it will answer instantly, confidently, and usually without telling you where the number came from. That confidence is the tell. Real dosing evidence is narrower than the forums suggest, and it comes in distinct tiers of certainty: things the FDA actually reviewed and approved, things one well-designed trial actually measured, things a meta-analysis found as a secondary effect, and things nobody has measured for you personally because they can’t be. Worth sorting those apart before trusting any figure.
Oral micronized progesterone is a prescription drug, approved by the FDA under the brand Prometrium [1]. Whatever dose fits a given person is a decision made by a licensed clinician who can see that person’s history and labs. This piece is not a substitute for that. It’s an audit of where the numbers actually come from.
Tier one: what the approved label actually says
The most solid ground here is the FDA-approved labeling for Prometrium. Not marketing copy, an approved document, reviewed by the agency, that specifies exact strengths and uses.
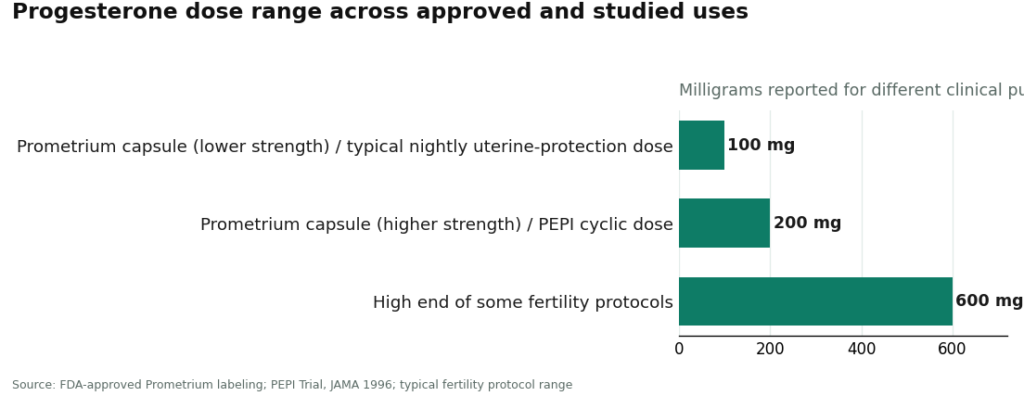
Two capsule strengths exist: 100 mg and 200 mg [1]. The label attaches them to two approved uses only: preventing endometrial hyperplasia in postmenopausal women with a uterus who are taking conjugated estrogens, and treating secondary amenorrhea, meaning periods that have stopped [1]. That’s it. That’s the entire footprint of what the FDA has actually signed off on. Everything else circulating online is extrapolation, sometimes reasonable extrapolation, but extrapolation nonetheless.
Tier two: one randomized trial, one specific number
The 200 mg figure that shows up constantly in dosing discussions has a real origin, and it’s worth naming precisely instead of treating it as folklore. It comes from the Postmenopausal Estrogen/Progestin Interventions trial, published in JAMA in 1996. Among its arms, postmenopausal women took cyclic oral micronized progesterone at 200 mg per day for 12 days each month, alongside estrogen. The unopposed-estrogen arm developed endometrial hyperplasia at much higher rates. The cyclic progesterone arm, like the other progestogen arms, kept hyperplasia close to placebo [2].
That is genuinely strong evidence, for exactly what it tested: a 12-day-a-month, 200 mg regimen, paired with estrogen, measured against endometrial hyperplasia as an outcome. It is not evidence for 200 mg daily, or 200 mg indefinitely, or 200 mg for anything other than that specific purpose. The trial answers a narrow question well. People keep asking it a broader one.
The reason clinicians treat this dosing question as non-negotiable rather than a nice-to-have optimization is spelled out in The North American Menopause Society’s 2022 position statement: hormone therapy risk depends on type, dose, route, timing, and whether a progestogen is used at all [3]. Under-dosing the progestogen isn’t a rounding error. It’s the difference between protecting the uterine lining and not.
The pattern matters as much as the number
A dose quoted without its regimen tells you almost nothing. Progesterone in menopause therapy generally runs one of two ways.
Cyclic (sequential) dosing means a higher dose for a set stretch of days each month, the PEPI pattern: 200 mg for 12 days [2]. It usually produces a scheduled withdrawal bleed, because the lining sheds when the progesterone phase ends.
Continuous combined dosing means a lower dose taken daily, alongside daily estrogen, aiming at the same protective goal through steady exposure rather than a monthly pulse, generally chosen to avoid that scheduled bleed.
So “200 mg” spoken in isolation could mean two different things depending on whether it’s a cyclic or continuous figure, and pretending otherwise is where a lot of the internet’s confidence goes wrong.
Tier three: a real but modest secondary finding
Bedtime dosing gets recommended constantly, and unlike a lot of dosing folklore, this one has an actual mechanism and an actual paper behind it. Oral micronized progesterone tends to cause drowsiness. Taking it at night works with that tendency instead of against it.
A 2021 systematic review and meta-analysis in the Journal of Clinical Endocrinology and Metabolism, drawing on randomized trial data mostly in postmenopausal women, found that micronized progesterone improved several aspects of sleep and self-reported sleep quality, though not uniformly across every measure [4]. That’s a real finding. It is also a modest one, observed within the context of menopause hormone therapy, not a standalone insomnia treatment. Treating this as license to take progesterone purely as a sleep aid outside a clinical indication would be reading more into the paper than it says.
Tier four: the question nobody’s data can answer
Here’s the honest limit, and it’s the one most confident dosing content quietly skips past. The label and the trials specify doses for defined populations tested for defined outcomes. None of them specify your dose. That isn’t a gap waiting to be filled by a better study. It’s structural.
Whether progesterone is even indicated depends on whether someone has a uterus. The correct dose depends on what estrogen they’re taking and at what level, whether the goal is endometrial protection or symptom relief or both, their menopausal stage, and how they individually tolerate and metabolize it. The North American Menopause Society states this plainly: hormone therapy decisions should be individualized [3]. A dose correct for one woman on one estrogen regimen can be wrong for another woman on a different one.
This is also where the approved-capsule-versus-compounded distinction stops being a regulatory footnote and becomes a dosing issue. The approved Prometrium capsule comes in fixed, manufactured strengths, 100 mg and 200 mg, with the dose consistency that an FDA-reviewed manufacturing process is supposed to guarantee [1]. Compounded progesterone can be custom-dosed, sometimes genuinely usefully when the commercial product doesn’t fit, but compounded preparations are not FDA-approved and are not reviewed by the agency for safety, effectiveness, or quality, including whether the dose in the capsule matches the dose on the label, before they reach a patient [5]. For a hormone whose entire endometrial-protection value depends on delivering a reliable dose, that’s not a small distinction.
How this actually plays out for a real patient
Since the “right dose” question can’t be answered by a chart, the practical question becomes who is deciding it and on what basis. In a supervised setup, a licensed clinician reviews the history, decides whether progesterone is indicated and why, chooses the form (approved capsule or compounded, on clinical grounds), sets the cyclic-or-continuous pattern, and a licensed pharmacy fills it. A provider such as FormBlends operates on that model, offering both the FDA-approved capsule and compounded versions and being clear about which is which, with the clinician making the call rather than a customer picking from a list.
Dosing also isn’t decided once and forgotten. Because hormone therapy gets reassessed over time, what a patient brings to a follow-up appointment shapes the next adjustment. Keeping a plain log of symptoms, sleep, and any bleeding between visits, something a tool like the FormBlends tracker app is built for, gives a clinician actual data instead of a vague recollection. That’s a logging aid, nothing more: not a prescription, not a diagnosis, not a substitute for the clinician doing the actual weighing.
The honest bottom line
There’s a small, specific set of progesterone doses the evidence actually supports, and each one belongs to a particular use. For endometrial protection in a woman with a uterus who’s on estrogen, the anchoring figure is the PEPI trial’s 200 mg cyclic dose for 12 days a month, because it’s the one shown, in a randomized trial, to keep hyperplasia near placebo levels [2], and the FDA label reflects that protective use [1]. Continuous combined regimens use a lower daily dose toward the same end. Bedtime timing has a genuine, if modest, basis in progesterone’s sedating profile and its documented secondary sleep benefit [4]. And beyond that, the data stops, deliberately, because the individual dose depends on variables only a clinician evaluating an actual patient can weigh [3]. A number without its indication, its regimen, and its population attached isn’t dosing information. It’s noise wearing the costume of precision.
Questions people actually ask
What dose does the FDA-approved label actually specify? Two manufactured strengths, 100 mg and 200 mg, tied to two approved uses: preventing endometrial hyperplasia in postmenopausal women on conjugated estrogens, and treating secondary amenorrhea [1]. That’s the full scope of what’s approved. Anything else is inference, not label content.
Where does the 200 mg number everyone quotes actually come from? The PEPI trial, which tested 200 mg of cyclic oral micronized progesterone for 12 days a month and found that arm kept endometrial hyperplasia near placebo while unopposed estrogen produced a large excess [2]. It’s a real, trial-derived number, but it’s a cyclic, 12-day figure paired with estrogen, not a universal daily amount.
What’s actually different between cyclic and continuous combined dosing? Cyclic dosing uses a higher amount for a set number of days each month, the pattern PEPI studied, and typically causes a scheduled monthly bleed [2]. Continuous combined dosing uses a lower daily amount alongside daily estrogen, aiming at the same protection without the scheduled bleed. Since the dose, schedule, and outcome all differ, a bare number without its regimen doesn’t tell you much.
Why does everyone say to take progesterone at night? Because it tends to cause drowsiness, so bedtime dosing works with that rather than against it. It also lines up with progesterone’s better-documented secondary benefit: a 2021 meta-analysis of randomized trial data found it improved several sleep measures, mostly in postmenopausal women [4]. That benefit is real but modest, and specific to menopause therapy, not a general case for progesterone as a sleep supplement.
Why does it matter whether the progesterone is the FDA-approved capsule or a compounded version? The approved capsule comes in fixed, manufactured strengths with the reliability an approved process is meant to ensure [1]. Compounded progesterone can be custom-dosed, which is sometimes genuinely necessary, but it isn’t FDA-approved and isn’t reviewed for safety, effectiveness, or dose consistency before it’s marketed [5]. For a drug whose protective effect depends on the dose actually being what the label says, that gap is a practical concern, not a technicality.
Can any general article tell me my correct dose? No, and that’s not a failure of the research, it’s the nature of individualized medicine. The right dose hinges on whether you have a uterus, what estrogen you’re on and at what level, whether the goal is protection or symptom relief, your menopausal stage, and your personal response, and the major guidance says explicitly that these calls should be individualized [3]. The trials tested defined populations for defined outcomes. They were never going to answer for you specifically.
What is progesterone and what does it actually do in the body?
Progesterone is a steroid hormone made mainly by the corpus luteum after ovulation and, during pregnancy, by the placenta. It preps the uterine lining for implantation, helps sustain early pregnancy, and works with estrogen to regulate the menstrual cycle. It also affects mood, sleep, and body temperature, which is why its swings across the cycle are noticeable to a lot of people.
What is progesterone used for medically, and does that differ from what’s sold as a supplement?
FDA-approved uses cover protecting the uterine lining in postmenopausal women on estrogen, supporting luteal-phase deficiency, and preventing preterm birth in certain high-risk pregnancies. “Progesterone cream” sold as a supplement is a different category entirely. Most over-the-counter creams contain little to no bioidentical progesterone at any meaningful concentration, and their claims don’t go through the FDA review a drug product does.
What dosage actually gets prescribed, and why the wide range?
Reported doses run from 100 mg nightly for uterine protection in menopause therapy up to 600 mg or more in some fertility protocols, numbers pulled from specific trial populations and specific endpoints, not interchangeable with each other. A prescriber’s target depends on why you’re taking it, your baseline hormone levels, the formulation, and how you personally absorb it. Oral progesterone gets heavily broken down on its first pass through the liver, so identical milligram doses can produce very different blood levels in different people.
Does progesterone cause weight gain?
The evidence is genuinely mixed, which is a more honest answer than a flat yes or no. Some people report bloating or fluid retention, especially at higher doses or with synthetic progestins, but well-designed trials of oral micronized progesterone haven’t consistently shown real weight gain. It can nudge appetite and fluid balance a little, and individual experience varies. Worth tracking alongside dose timing and discussing with a prescriber rather than assuming one causes the other.
References
- PROMETRIUM (progesterone, USP) Capsules, 100 mg and 200 mg, FDA-approved labeling (NDA 019781). Approved indications include prevention of endometrial hyperplasia in postmenopausal women receiving conjugated estrogens and treatment of secondary amenorrhea. U.S. Food and Drug Administration, Drugs@FDA labeling. https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/019781s013lbl.pdf
- The Writing Group for the PEPI Trial. Effects of hormone replacement therapy on endometrial histology in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA, 1996. Cyclic oral micronized progesterone 200 mg/day for 12 days a month kept endometrial hyperplasia rates near placebo, while unopposed estrogen produced a large excess. https://pubmed.ncbi.nlm.nih.gov/8569016/
- The North American Menopause Society. The 2022 hormone therapy position statement of The North American Menopause Society. Menopause, 2022. Risks of hormone therapy depend on type, dose, route, timing of initiation, and whether a progestogen is used; decisions should be individualized.
- Nolan BJ, Liang B, Cheung AS. Efficacy of Micronized Progesterone for Sleep: A Systematic Review and Meta-analysis of Randomized Controlled Trial Data. Journal of Clinical Endocrinology & Metabolism, 2021. Micronized progesterone improved several aspects of the sleep cycle and self-reported sleep, predominantly in postmenopausal women.
- U.S. Food and Drug Administration. Compounding and the FDA: Questions and Answers. Compounded drugs are not FDA-approved, meaning the agency does not review their safety, effectiveness, or quality before they are marketed; compounded drugs can serve important medical needs.
Written by Noah Farrell, features writer. Reviewing the trials and labels directly. Last reviewed March 2026.
Not a substitute for medical care. Bring any new treatment idea to your healthcare provider first.

 By
By